An assessment of COVID vaccine coverage in 2020 - 2022
—> 80% (*) chance of a US vaccine approval by year end 2020
—> 60% chance that the US will have enough supply of vaccine to cover the country by mid 2021
—> 60% chance significant part of world is covered by early 2022
(* This estimate dipped in Sep but has rised by Nov, and should probably now nudge 90% for Dec/Jan approval due to both Pfizer and Moderna vaccines hitting)

Table 1. Source: Milken Institute, Press Releases, Author estimates. No approvals are certain. One vaccine in Russia and one vaccine in China have been approved for certain use.
I estimate an 80% chance of a vaccine approval by year end 2020 and a 60% chance that the US will have enough supply of vaccine to cover the country in first wave by mid 2021. (Although note as counter point on the safety risk you can note this article on the 1976 Swine flu).
The base case uses the public announcements of the large sophisticated UK and US groups. (See Table above).
Downsides are from (1) negative data and (2) negative regulators; other possible downside are from (3) manufacturing constraints and (4) distribution constraints; and (5) vaccine hesitancy (certain anti-vaccine sentiments). Note (1) and (2) are separate risks as there may be data positive enough for patient choice (or developers to submit) but not enough to convince (risk averse) regulators.
Upsides are from (a) China developers and possibly (b) Russian development although I do not see those vaccines coming to Europe or the US but may well go to Asia and LatAm in H2 2021. A detailed overview of the developer groups is available from the the Milken Institute (link end) and WHO. I select a highlight below to give a sense of (i) the variety of technology mechanisms in play here and (ii) the colloborative group nature of the development even while there typically is a lead group.

Source: Milken Institute, slight author edits.
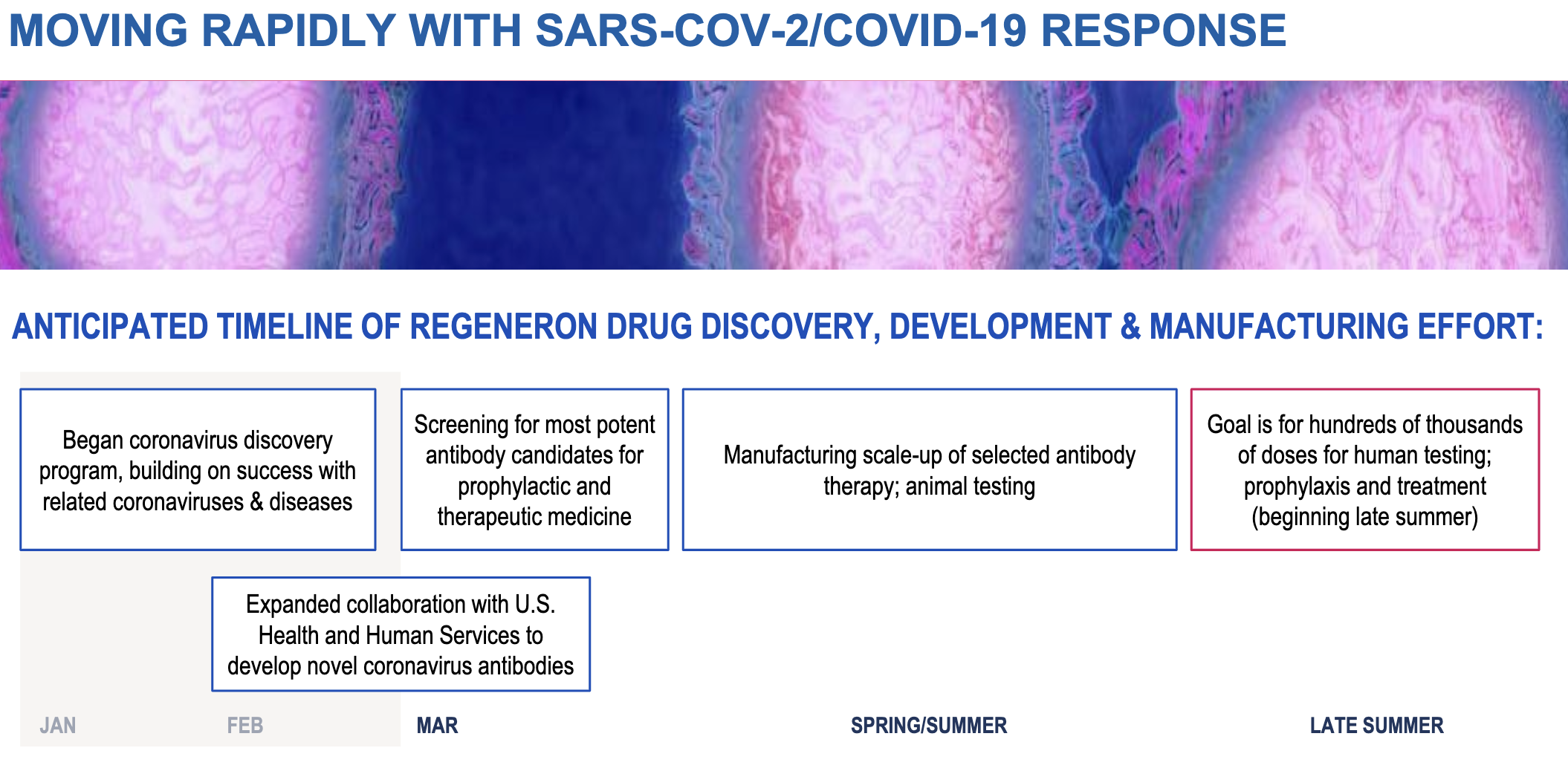
Further upside would be positive data from manufactured antibody studies (eg Regeneron/Roche) which are due Q4 2020. The two major studies due in Q4 2020 are (a) Regeneron/Roche and (b) Lilly/AbCellera. If these are positive, then the Regeneron collaboration would add 4m to 8m prevantative doses to the calculations below.
I am less worried about distribution because:
—>vaccination during the flu season routinely reaches 50% of the population, thus distribution efforts are likely surmountable (cf US wholesaler deal with McKesson which is an experienced organisation). Also fill/finishers (packing the finished product) such as Catalent are already involved.
—> some nucleic-acid based vaccines may be distributed frozen, but appear stable for several days in regular refrigeration
The leading makers are also fully flying on manufacturing and there is expertise from flu vaccine and animal vaccines and outsourced makers (eg Lonza). I have toured vaccine plants (which are typically under utilised compared to chemical plants) and the technology and expertise from the leading makers is competent at scale, although this current speed is much faster than before - in my view, it’s not been out of reach for biopharma.
There are previous papers on biopharma probability of success. And while certain technology is new eg mRNA-based vaccines, much of the expertise on coronavirus and vaccine understanding has a high degree of understanding. Severe side effects (or long-term side effects) are risks (particularly from our understanding of side effects from previous RSV vaccines) but current data from multiple trials are not yet picking up a nasty effect. Although the trials are small, and many are across different products, the fact that there are multiple trials running across different geographies and populations gives statistical strength to the net probability of success. (Link end, see my primer on forecasting).
Some vaccines will fail. Some supply bottlenecks will materialize. New bottlenecks, so far undiscovered will appear. But the net effect of so many shots on goal is that a first wave of vaccinations can be done in the US by mid 2021 and quite likely globally by end 2021 / early 2022. The stated capacity up to 1bn doses of many of the possible successes balances out those vaccines that will fail.

Source: Author estimates, Company Press releases, transcripts of managment calls. This table looks only at US, however similar calculation can show reasonable global coverage by mid 2022. Note, vaccination = 2 x doses in most cases as two doses required.
There will need to be boosters (maybe every 2 years, possibly every year) and possibly - like flu - new strains will have to be made yearly if the virus ends up mutating and still being lethal, but my view is that we now are looking pretty likely to be on track to solving this one.

Source: Milken Inst, Press releases, Author estimates. Note: Private funding may not be but have not assertained. DOD = Dept of Defence, HHS = Human Health Services. BARDA = Biomedical Advanced Research and Development Authority. CEPI = Coalition for Epidemic Preparedness Innovations . EC = EU Commission. EIB = EU Investment Bank. GAVI = Vaccine Alliance. GAtes = Bill and Melinda Gates Foundation.
While there will be many debates on the public health responses of various countries, it’s notable that the US, China and the UK are the geographies where the developing makers are concentrated with honourable mentions to a few countries such as France (Sanofi) and maybe Germany (CuraVax). Adjusting for population keeps UK in the spotlight (note Tyler Cowen has highlighted this in his column, link end).
Understanding this is insightful as the observation centres around historic expertise in vaccines and biological manufacturing capability from GlaxoSmith Kline, AstraZeneca and the Jenner Institute (Oxford University). There is a learning here too for the unfortunate circumstance of much of biopharma closing down antibiotic research (in reality because of lack of commerical markets arguably due to inability to be able to price effectively as generics for old drugs are cheap and systems won’t pay enough for novel antibiotics).
After arguably a slightly slow start US government, the BARDA programme, looks fairly effective and the US biopharma response across the spectrum has been pretty good (I’d also include most global biopharma where they have expertise eg Roche partnered with Regeneron as well as executing on diagnostics, Novartis where it had technology (hydroxychloroquine).
China is hard to assess sitting at a desk outside China, but impressions also seem favourable given they have many shots in the leading group and the sheer number of smaller biotechs working in the area (see Milke Institute tracker) is large at earlier stage.
Overall, this to me looks like a win for science and innovation and perhaps shows we as humans can still build things (fairly fast) when needed.
Background assumptions to consider:
Vaccine developers will begin delivery of vaccine at the earliest possible date of approval and deliver the purchased amount over 6 months. The exception to this logic is AstraZeneca where the purchase volume is significantly greater (although the terms of the agreement are unclear).
There is an adjustment from 'doses' to 'vaccinations' based on whether each vaccine will require a second dose (booster). Immunogenicity data from Pfizer, Moderna, AstraZeneca and Novavax all suggested that that a booster will likely be required.
Limited EUA (emergency use authorisation) will likely prevent supply shortage even early on. If vaccines were approved for the entire US population in late 2020, there would be shortages until March 2021. Still this seems unlikely. The initial market entry based on EUA will be based on convincing efficacy data. In contrast, safety data will be broad (10,000s patients) but of relatively short duration, as the trials are expected to accumulate events (infections) quickly.
Given political pressures, historic risk aversion when full data lacking (also note recent complete response letters to novel treatments eg gene therapy haemophilia, JAK inhibitor, in Q2 / Q3 2020) FDA would limit the use to high-need groups (essential employees, high-risk comorbidities). If this is the case, then pre-approval manufactured amounts will be sufficient to satisfy demand.
I would still support informed patient choice in this scenario (see my previous paper) but I doubt we will have it.
Links:
My forecasting Primer including on drug probabilty forecasting.
My early vaccine use idea based on patient choice.
Tyler Cowen on UK COVID response.